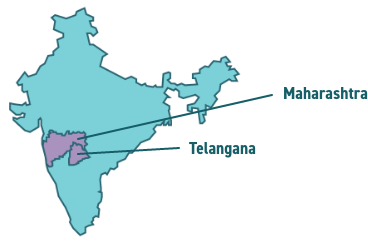
Current outbreak of chikungunya
Maharashtra and Telangana, India (as of December 19, 2024)

Evidence of transmission within the last 5 years
Current outbreak of chikungunya
Maharashtra and Telangana, India (as of December 19, 2024)
Evidence of transmission within the last 5 years
The Caribbean was the most likely source region for diagnoses of chikungunya.13
Half of ill-returned travellers with chikungunya acquired the infection during trips of ≤2 weeks duration.13
89% of ill-returned travellers with chikungunya had a musculoskeletal-presenting complaint, while only 54% reported fever as their presenting symptom, and 30% complained of a chikungunya-associated rash.13
41 (34.7%) ill-returned travellers with chikungunya presented for care at a CanTravNet site within 28 days of travel, while 28 (23.7%) presented ≥60 days post-travel, and 16 (13.6%) presented ≥90 days post-travel, supporting that many travellers presented for care of chronic arthropathic symptoms.4,13,14
Co-infections, which may have overlapping or entirely different symptoms to chikungunya, may complicate the initial diagnostic assessment.13